// 04 — Reimagining Recovery
The full model at a glance
Core theory, multi-theory lens, and the three-year PhD research roadmap — condensed into one map.
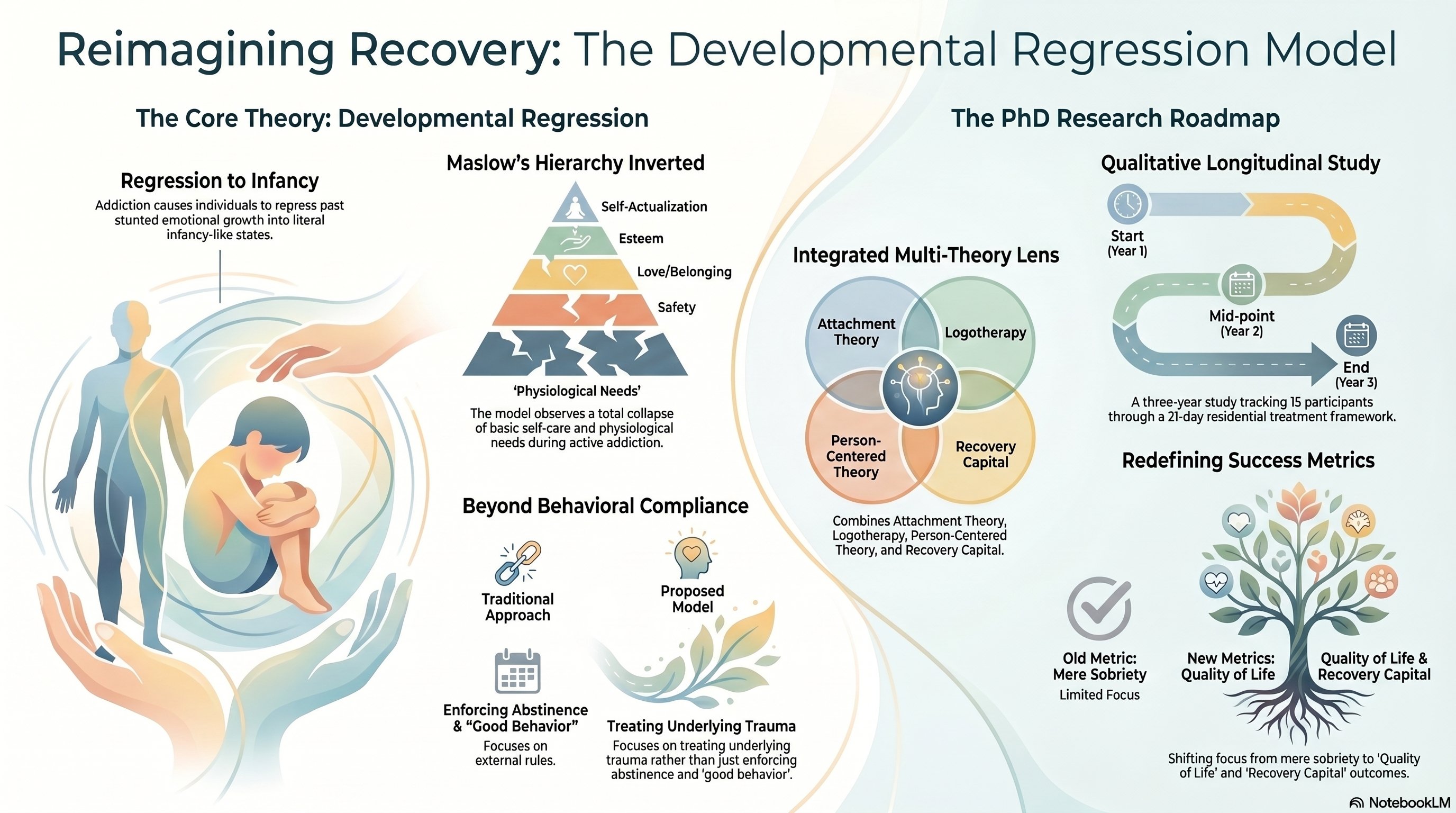
A trauma-first reframe of addiction recovery — testing the hypothesis that the Jellinek progression of addiction is Maslow's hierarchy collapsing in reverse, and that rebuilding recovery capital must start at the foundation, not the roof.
youtu.be/uNeioNCFwNg
youtube.com/live/E6tsry1zdcQ
Addiction doesn't just stunt emotional growth — it collapses the hierarchy of needs floor by floor, until the individual is operating from a state of total dependency, just like an infant.
Abandoning passions and purpose.
Isolation, destruction of relationships, overwhelming shame.
Ignoring physical health, nutrition, and basic human maintenance.
The state requiring total external management to survive.
| Dimension | Traditional addiction treatment | The developmental regression model |
|---|---|---|
| View of the patient | A poorly behaved, willful individual requiring discipline. | A traumatized individual relying on faulty, early-life coping mechanisms. |
| Metric of success | Complete abstinence and behavioral compliance. | Rebuilt quality of life and the measurable accumulation of Recovery Capital. |
| Core modality | Shame, punishment, and managing surface-level symptoms. | Establishing a Secure Base, fostering loving responsibility, and treating underlying trauma. |
The model isn't theory borrowed from a textbook — it's drawn from a life that travelled through the territory it describes, and then earned the clinical language to map it.
First experiences of trauma and self-harm. Later studies a BSc in Psychology before pivoting to counselling.
Substance use disorder peaks; an overdose with a near-zero chance of survival precedes entry into rehab. Hired the same year at a clinic immersed in the abstinence-based Minnesota model.
Achieves a Bachelor of Social Work; works as a registered clinical practitioner bridging lived empathy with clinical expertise.
Core theory, multi-theory lens, and the three-year PhD research roadmap — condensed into one map.
A medically licensed residential detox and treatment facility in South Africa runs the standard 21-day program — 3 days of medical detox followed by 18 days of primary care. This is the critical window for first intervention.
South Africa's profound legacy of widespread trauma makes it a crucible: a model that rebuilds trust and recovery capital here should be robust enough for global export.
5 per year, tracked across the full three-year study.
The residential window dictated by medical aid constraints.
Start, mid-point, and end of the qualitative longitudinal study.
Strict patient anonymity, total research transparency, and careful navigation of the dual social worker / researcher role.
Robust case management, backed by internal and international case review boards operating weekly.
A clinical psychologist, a registered counsellor, trauma specialists, nursing staff, and a personal clinical supervisor.
An academic application for a Master's was assessed as PhD-level work — and put into abeyance rather than diluted. The search now is for a supervisor who understands the fusion of lived experience, social work, and addiction.
An academic supervisor to guide rigorous academic writing and qualitative data structuring — without the risk of institutional dilution.
Strong interest in cross-border supervision, including alignment with work on gender-based violence and the Recovery Resilience Facilitators programme.
This is not about earning a title. It is about rigorously testing a clinical breakthrough so we can stop punishing symptoms — and start rebuilding human lives, worldwide.